

Abstract
Introduction: Red blood cell (RBC) alloimmunization is an important transfusion complication which is very prevalent among patients with sickle cell disease (SCD). Only part of patients is able to develop alloantibodies following antigen-mismatched transfusions, named the 'immune responders', who should be prospectively transfused with antigen-matched RBC units, comprising the most immunogenic erythrocyte antigens. Auto-immune diseases are a known risk factor for RBC alloimmunization, suggesting that auto-immunity and post-transfusion alloantibody development happen through similar physiopathological pathways. In this context, polymorphisms in FCGR2B gene have already been associated with several auto-immune disorders and, hypothetically, could be associated with RBC alloimmunization and help to identify the 'immune responders' in transfusion practice.
Methods: In this case-control study, we enrolled 277 transfused SCD patients with retrospective data on alloimmunization status and transfusion exposure from two Brazilian centers. DNA samples (collected from March, 2017 to June, 2018) were extracted from whole blood samples using commercial kits (PureLink™ Genomic DNA®, Invitrogen, CA), and used for PCR amplification of promoter region of FCGR2B gene containing both -386G/C and -120T/A single nucleotide polymorphisms (SNPs) using gene-specific primer. SNPs of the FCGR2B were genotyped by direct Sanger sequencing (ABI3730XL, Applied Biosystems, CA). Cases had a positive history of alloimmunization with a clinically significant alloantibody and a minimum transfusion exposure of 1 RBC unit. Controls had a negative history of alloimmunization and having received ≥ 2 RBC units. Patients with autoimmune diseases or poor quality of DNA were excluded. Unadjusted and adjusted analyses were conducted by using Logistic Regression models to determine the association of covariates with binary outcome. Since the assumption of linearity in the logit was not supported, continuous covariates were categorized based on optimum cut-off point derived from ROC analysis. All statistical analyses were performed using SAS University Edition. A p-value of <0.05 was considered to be statistically significant.
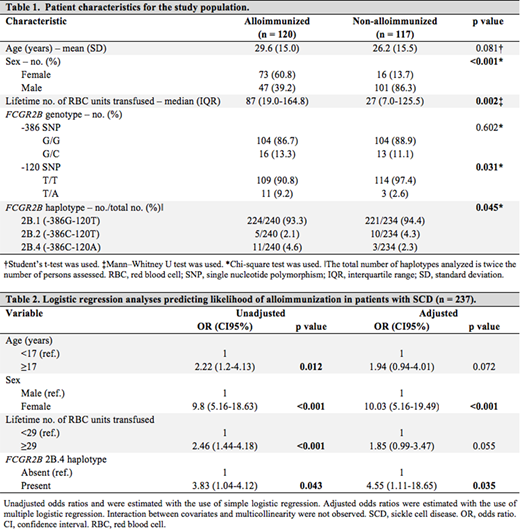
Results: A total of 237 patients met the eligibility criteria, 121 cases (alloimmunized) and 117 controls (non-alloimmunized). Majority of patients were female in cases (61%) and male in controls (86%), with mean age of 27.9 years (SD 15.3). Table 1 list the characteristics between the groups. RBC alloimmunization was associated with female sex (p<0.001), lifetime number of RBC units transfused (p=0.002) and FCGR2B 120T/A SNP (p=0.031). No statistically differences in the allele frequency of c.386C were observed between groups (p=0.602). FCGR2B -386G/C and -120T/A SNPs were in intense linkage disequilibrium. Three haplotypes of promoter region were identified as 2B.1 (-386G-120T), 2B.2 (-386C-120T) and 2B.4 (-386C-120A) with statistical significance (p=0.045). Logistic regression model was performed to assess the effects of age, gender, lifetime number of RBC units transfused and FCGR2B 2B.4 haplotype on the likelihood of RBC alloimmunization in patients with SCD. The analysis identified that female sex (OR 10.03, CI95% 5.16-19.49; p<0.001) and FCGR2B 2B.4 haplotype (OR 4.55, CI95% 1.11-18.65; p=0.035) predict increased risk of RBC alloimmunization in SCD patients as show in Table 2.
Conclusions: SCD patients with the FCGR2B 2B.4 haplotype had over a 4-fold higher risk for RBC alloimmunization in comparison with patients without this haplotype and probably may be helpful to identify the 'immune responders'. The presence of FCGR2B 2B.4 haplotype have been associated with increased expression of this inhibitory Fc gamma receptor in immune system cells, that was strongly associated with capacity of immune tolerance, regulating the development of antibodies. Future studies are needed to understand more about the functional and immune mechanism behind alloimmunization in SCD patients and ultimately improve our current preventive strategies.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal